

Research & Data
IOTA Dashboard brings kidney transplant performance data into focus
In July 2025, the Centers for Medicare & Medicaid Services (CMS) launched the Increasing Organ Transplant Access (IOTA) Model, a mandatory six-year initiative aimed at increasing kidney transplants and improving quality of care. Half of U.S. kidney transplant hospitals were randomly selected to participate, with the other half serving as the comparison group.
To support implementation, UNOS developed the IOTA Dashboard. The tool helps transplant hospitals monitor performance metrics, forecast expected points, and track progress toward IOTA’s three goals:
- Maximizing the use of deceased donor kidneys
- Improving care before, during and after kidney transplants
- Reducing disparities in transplant access and outcomes
Performance year 2 data is now available on the IOTA Dashboard.
A timesaving tool for transplant teams
For Joshua Liggett, transplant quality specialist and applied anthropologist at UC San Diego Health, the dashboard has been a great timesaver.
“This is a fantastic tool,” he said. “It’s so concise, and it puts everything together in such a digestible way to provide a pulse of where we stand on IOTA.”
Liggett uses the dashboard during meetings with UC San Diego’s kidney transplant program leaders and during monthly Quality Assessment and Performance Improvement meetings with interdisciplinary teams. The program pairs the IOTA Dashboard with Scientific Registry of Transplant Recipients’ CUSUM and annual reports to estimate its efficiency score.

“This is a fantastic tool It’s so concise, and it puts everything together in such a digestible way to provide a pulse of where we stand on IOTA.”
—Joshua Liggett, transplant quality specialist and applied anthropologist at UC San Diego Health
Reducing the burden of metric tracking
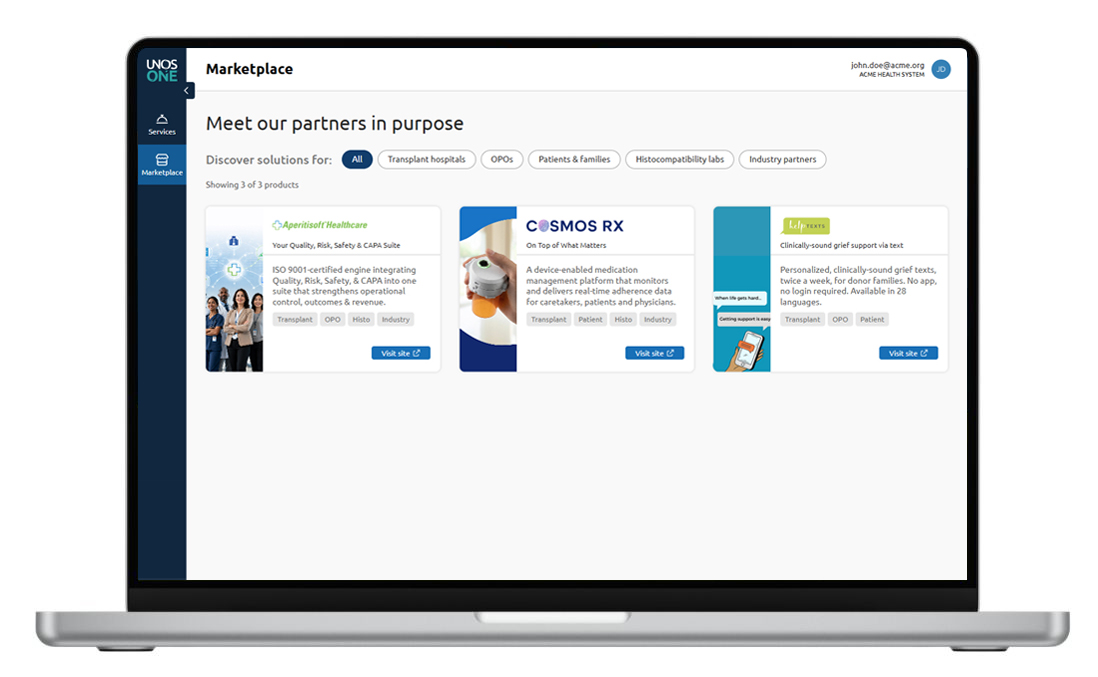
When UC San Diego Health first learned it had been selected for the IOTA Model, staff were concerned about the administrative burden of tracking the metrics. The IOTA Dashboard reduces that burden by consolidating performance data and clearly displaying scores across each domain. Instead of consulting multiple databases and building presentation slides, Liggett said he can simply share a screenshot of the IOTA Dashboard.
“That’s resource time that can be used on other projects,” he said.
The IOTA Dashboard has also helped UC San Diego Health identify opportunities to improve organ use and patient care.
“We need to be using as many organs as we possibly can to keep our achievement volume up,” he said. “It prompted us to take a look at some of our internal treatment protocols for different types of patients. Maybe we treat our patients in a different way post-transplant to maximize their survival and make sure that they have a good post-transplant experience.”
Useful beyond IOTA participation
Liggett believes the IOTA Dashboard is a valuable tool even for hospitals that are not participating in the IOTA model.
“Everybody should be using it,” he said. “Even if you are not an IOTA participant, it’s still a helpful tool to measure these three critical things.”

UNOS insights and analysis on healthcare and transplant issues